Anterior Uveitis
Definition & Pathogenesis
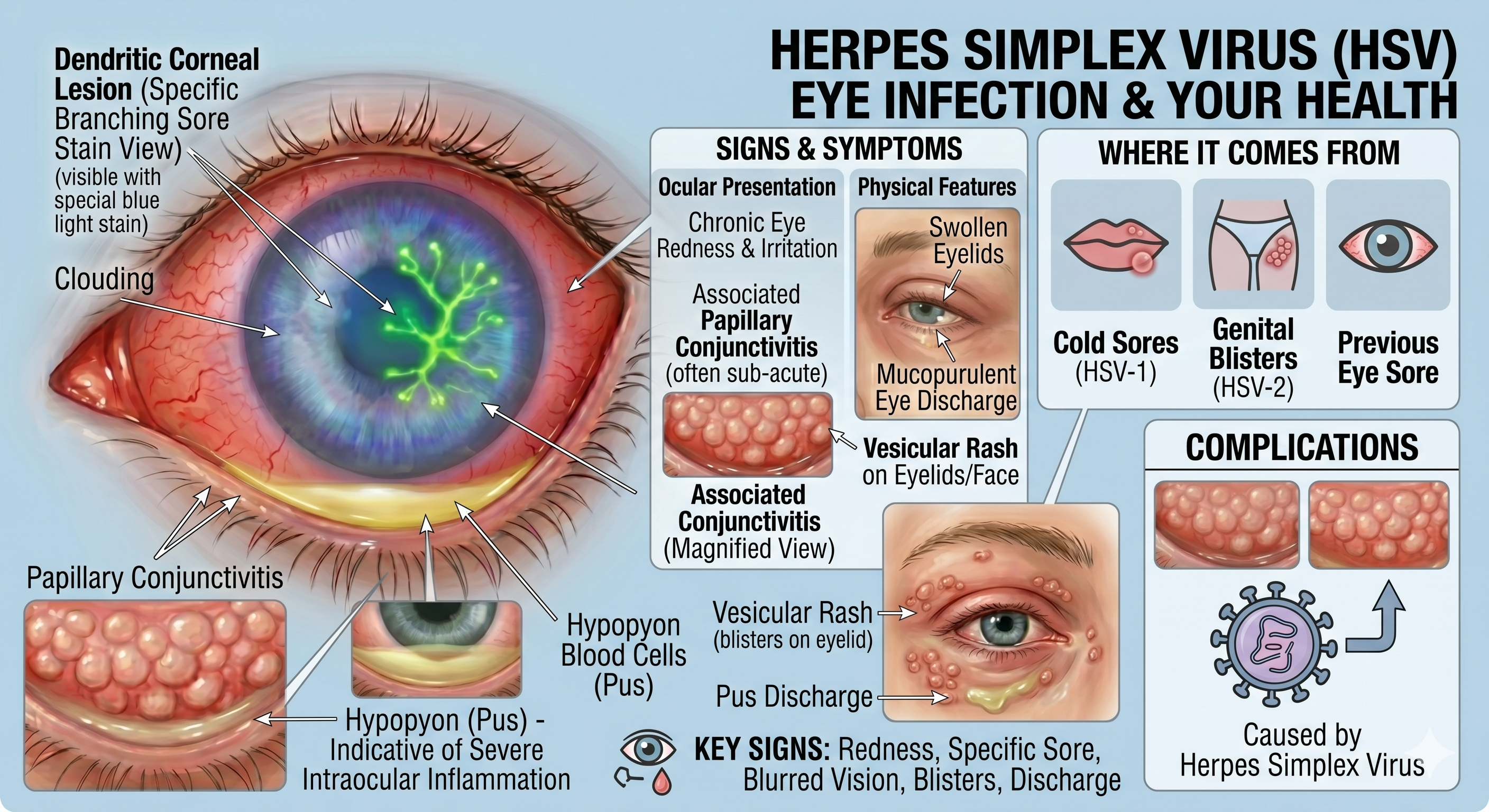
A viral infection caused by the Herpes Simplex Virus (HSV) that leads to a
chronically red and irritated eye.
● It primarily produces characteristic dendritic lesions on the corneal epithelium.
● Patients often have a history of cold sores, genital herpes, or previous keratitis. It
can become exceptionally severe in atopic patients (a condition called eczema
herpeticum).
Signs & Symptoms
● Ocular Presentation: Redness, irritation, and dendritic corneal ulcers (which
become visible when using fluorescein dye and blue light). A hypopyon (pus)
may appear if there is intraocular inflammation.
● Physical Features: Swollen eyelids, eye discharge, associated papillary
conjunctivitis, and a vesicular rash on the face or eyelids (often preceded by a
24-hour tingling sensation).
.
Key Diagnostic Signs
Clinicians look for several specific markers within the eye to confirm the diagnosis
● Ciliary Injection: A deep, purplish redness around the edge of the cornea.
● Pupillary Changes: The pupil is often constricted (miosis) due to muscle spasms.
● Anterior Chamber Activity:
○ Cells and Flare: Floating white blood cells and a “foggy” appearance (flare)
caused by protein leakage.
○ Hypopyon: A visible layer of white inflammatory cells that settles at the bottom of the anterior chamber.
● Keratic Precipitates (KP): Clusters of inflammatory cells that stick to the inner surface of the cornea.
Iris and Structural Changes
If left untreated or in chronic cases, the iris can undergo significant changes
● Posterior Synechiae: The iris becomes “stuck” to the lens behind it.
● Iris Nodules: Small lumps (Koeppe or Busacca nodules) appearing on the surface or margin of the iris.
● Atrophy and Color Shifts: The iris may thin or change color (heterochromia).
● Rubeosis Iridis: The growth of abnormal new blood vessels on the iris.
Intraocular Pressure (IOP)
The pressure inside the eye is unpredictable. It may be abnormally low because the eye’s fluid production is “shut down” by inflammation, or it may be abnormally high due to debris blocking drainage or as a side effect of steroid treatment.
Primary Treatment Pillars
● Topical Steroids: The “gold standard” first-line therapy (e.g., prednisolone or dexamethasone). Treatment is usually intensive initially—often one drop every hour—and then carefully tapered over 5 to 6 weeks to prevent a relapse.
● Cycloplegic Agents: Medications like atropine or cyclopentolate are used to
paralyze the ciliary muscle. This relieves painful muscle spasms and prevents
the iris from sticking to the lens (posterior synechiae).
Advanced Interventions For cases that are severe, resistant, or complicated, several targeted procedures may be used:
● Mydricaine No. 2: Administered via injection or a soaked cotton pledget to break
fresh, stubborn adhesions.
● Tissue Plasminogen Activator (TPA): Injected directly into the eye to dissolve
thick, fibrous clots (fibrinous exudates).
● Regional Steroid Injections: Injections around the eye (sub-Tenon or
transseptal) used for patients who struggle with drops or those developing
macular swelling.
● Intraocular Steroids: Injections directly into the vitreous for macular oedema
that doesn’t respond to other treatments
Systemic & Chronic Management
● Alternative Medications: If topical drops are inadequate, systemic steroids,
NSAIDs, or antimetabolites (like methotrexate) may be used as “steroid-sparing”
measures for chronic conditions.
● Targeted Therapy: If the uveitis is triggered by an underlying infection, specific
antimicrobial therapy must be used alongside anti-inflammatory treatment.
Key Takeaway: Consistent tapering of steroids is essential to ensure the inflammation is fully suppressed and does not return immediately after treatment ends.