Treatment
The primary goal in the treatment of glaucoma is to lower the intraocular pressure (IOP) to a “target pressure” to prevent further damage to the optic nerve. According to the provided resources, management is categorized into medical, laser, and surgical interventions.
Medical Treatment
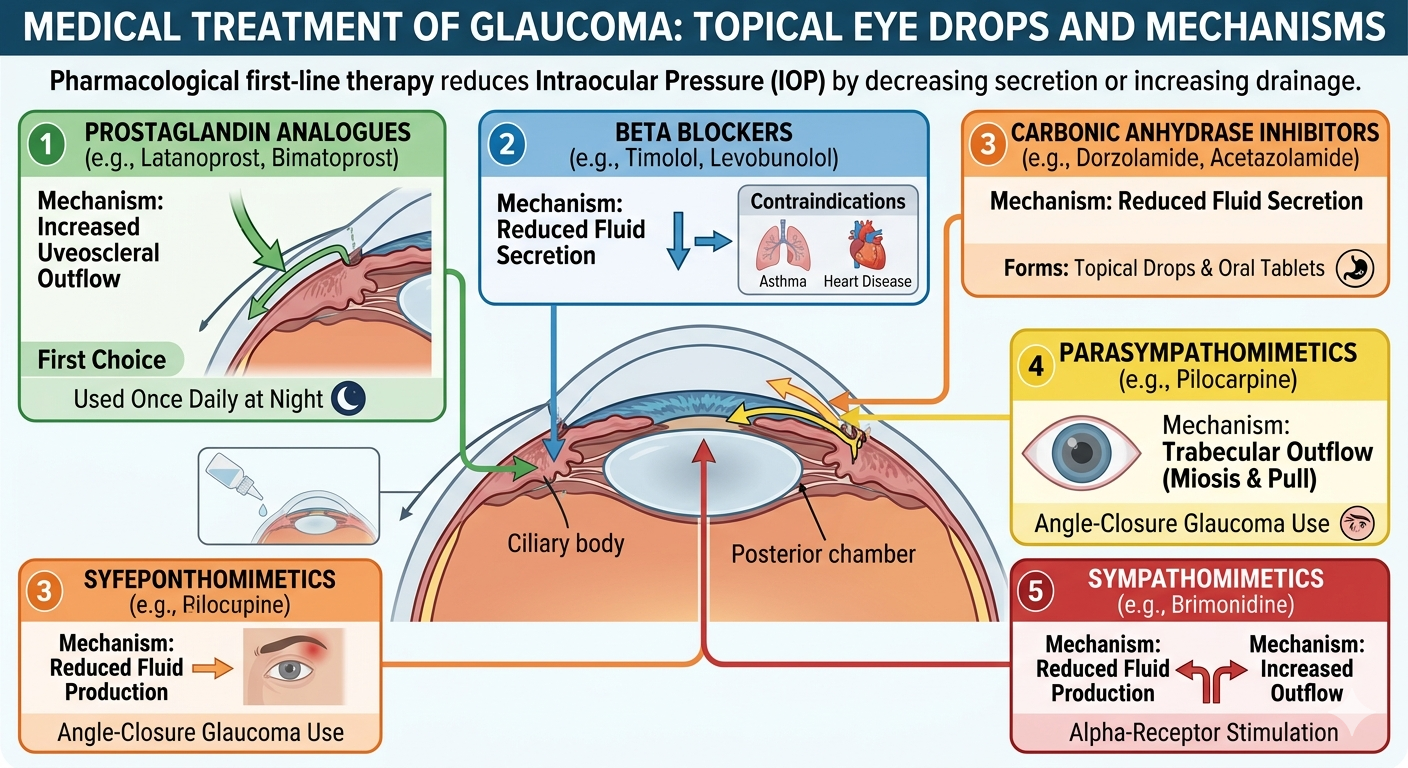
Topical eye drops are the most common first-line therapy.
- Prostaglandin analogues (e.g., latanoprost, bimatoprost): These are often the first choice because they are effective at reducing IOP by increasing aqueous outflow through the uveoscleral pathway. They are typically used once daily at night.
- Beta blockers (e.g., timolol, levobunolol): These reduce the secretion of aqueous humor. They are contraindicated in patients with a history of heart or lung disease, such as asthma.
- Carbonic anhydrase inhibitors (e.g., dorzolamide, acetazolamide): These also reduce the secretion of aqueous humor. They are available as topical drops or oral tablets, though the systemic form may cause side effects like nausea and electrolyte disturbances.
- Parasympathomimetics (e.g., pilocarpine): These constrict the pupil and pull on the trabecular meshwork to increase drainage. They are useful in angle-closure glaucoma but may cause side effects like brow ache.
- Sympathomimetics (e.g., brimonidine): These stimulate alpha-receptors to reduce fluid production and increase outflow.
Laser Treatment
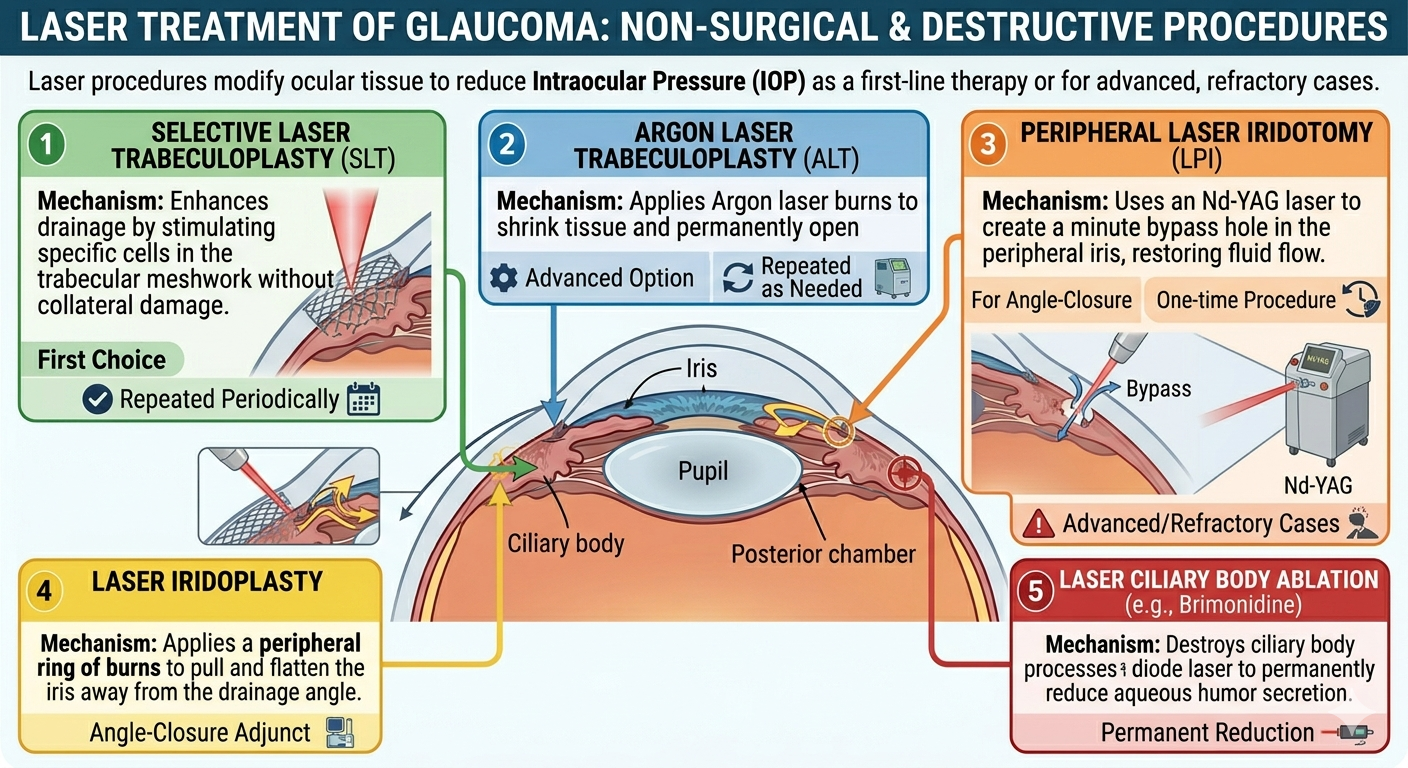
Laser procedures are used when medical therapy is insufficient or as an alternative to surgery.
- Laser trabeculoplasty: Applied to the trabecular meshwork to open drainage channels in open-angle glaucoma.
- Peripheral laser iridotomy: A hole is cut in the peripheral iris using an Nd-YAG laser to restore fluid flow in angle-closure glaucoma.
- Laser iridoplasty: A ring of burns is applied to the peripheral iris to pull it away from the drainage angle.
- Laser ciliary body ablation: The ciliary body is destroyed using a diode laser to permanently reduce fluid production, usually reserved for advanced or refractory cases.
Surgical Treatment
Surgery is indicated when IOP cannot be controlled with drops or lasers.
- Trabeculectomy: This is the “gold standard” drainage operation. It creates a guarded channel that allows aqueous to flow from the anterior chamber into the sub-Tenon’s and subconjunctival space, forming a drainage bleb.
- Anti-scarring agents: Drugs like 5-fluorouracil or mitomycin C are used during or after surgery to prevent the drainage site from scarring shut.
- Drainage shunts (Tubes): Devices such as the Ahmed or Baerveldt implants are used in complex cases like neovascular glaucoma. A tube is inserted into the anterior chamber to drain fluid to a reservoir behind the eye.
- Minimally invasive glaucoma surgery (MIGS): Newer, less invasive surgical options that offer improved safety profiles compared to traditional filtering surgery.
- Non-penetrating surgery: Includes procedures like deep sclerectomy and viscocanalostomy, which reduce IOP without fully penetrating the anterior chamber.
Emergency Treatment: Acute Angle-Closure Glaucoma
Acute angle-closure glaucoma is an ophthalmic emergency requiring rapid medical reduction of IOP.
- Intravenous acetazolamide (500 mg) is given to lower pressure quickly.
- Pilocarpine (4%) is instilled to constrict the pupil and pull the iris away from the drainage angle.
- Definitive treatment is a peripheral iridotomy or iridectomy.