Major Classifications
Based on the mechanism of the drainage obstruction, glaucoma is generally classified as:
- Primary Open-Angle Glaucoma (POAG): The drainage angle remains open, but resistance to fluid outflow through the trabecular meshwork gradually increases. This is often asymptomatic until late stages.
- Primary Angle-Closure Glaucoma (PACG): The iris is pushed or pulled against the trabecular meshwork, physically blocking the drainage angle. This can occur suddenly as a painful medical emergency.
- Normal-Tension Glaucoma (NTG): A variant where glaucomatous optic nerve damage and visual field loss occur despite IOP measurements staying within the statistically “normal” range (below 21 mmHg).
- Secondary Glaucoma: Damage resulting from other ocular or systemic conditions, such as uveitis (inflammatory glaucoma), trauma, or diabetes (neovascular glaucoma).
- Primary Congenital Glaucoma: Caused by an abnormally developed trabecular meshwork at birth.
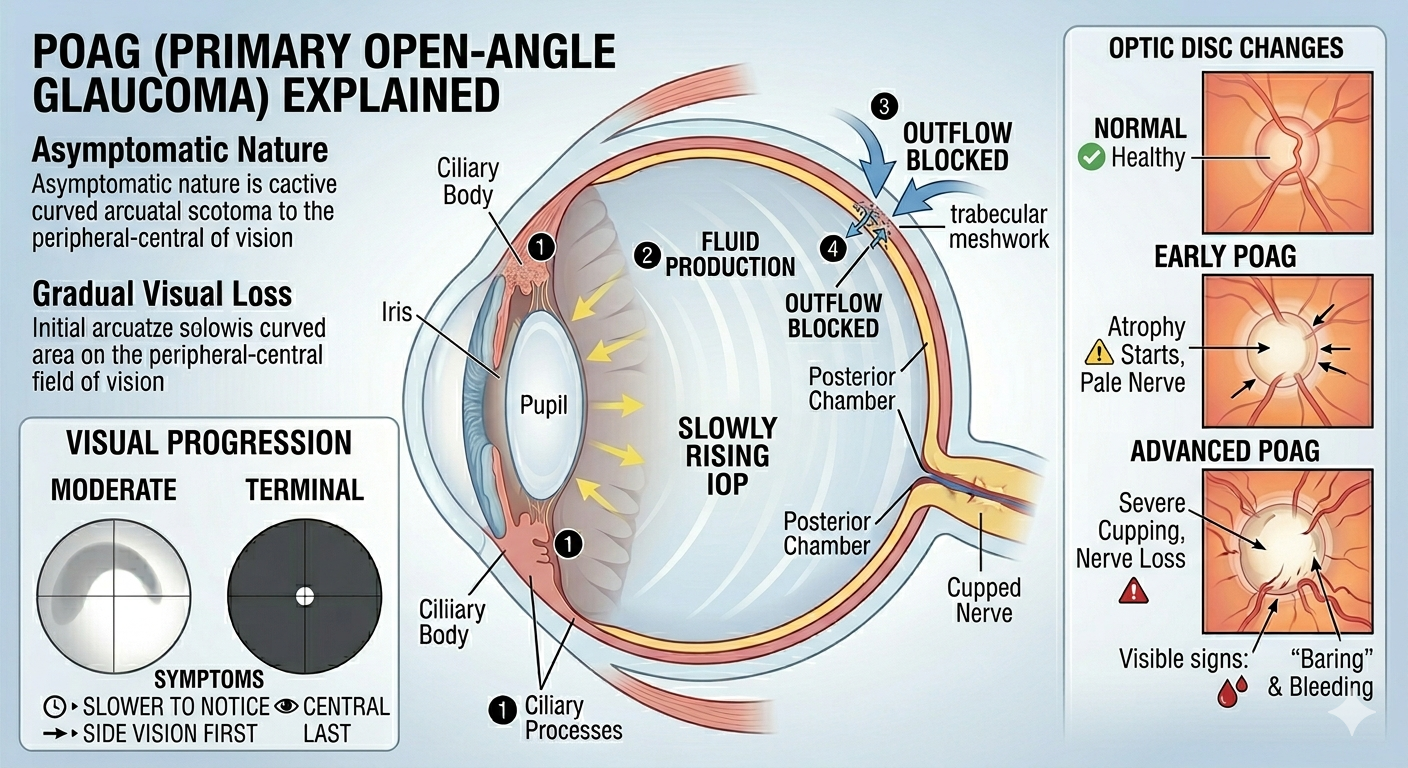
Primary Open-Angle Glaucoma (POAG)
This is a chronic condition where the intraocular pressure usually rises slowly.
- Asymptomatic Nature: Patients typically do not notice any symptoms until severe visual damage has occurred.
- Gradual Visual Loss: Vision impairment is slow and progressive.
- Optic Disc Changes:
- The optic disc appears pale and “cupped” as nerve fibers atrophy.
- An increased cup-to-disc (C/D) ratio (e.g., >0.3).
- Asymmetry in cupping between the two eyes.
- Disc haemorrhages may be present.
- “Baring” of vessels and “kinked” vessels at the edge of the optic disc.
- Visual Field Defects:
Initial loss typically presents as an arcuate scotoma (a curved area of loss that arches over central vision to the blind spot).
-
- Tunnel Vision: In terminal stages, central vision (6/6) may be preserved while the peripheral field is severely contracted.
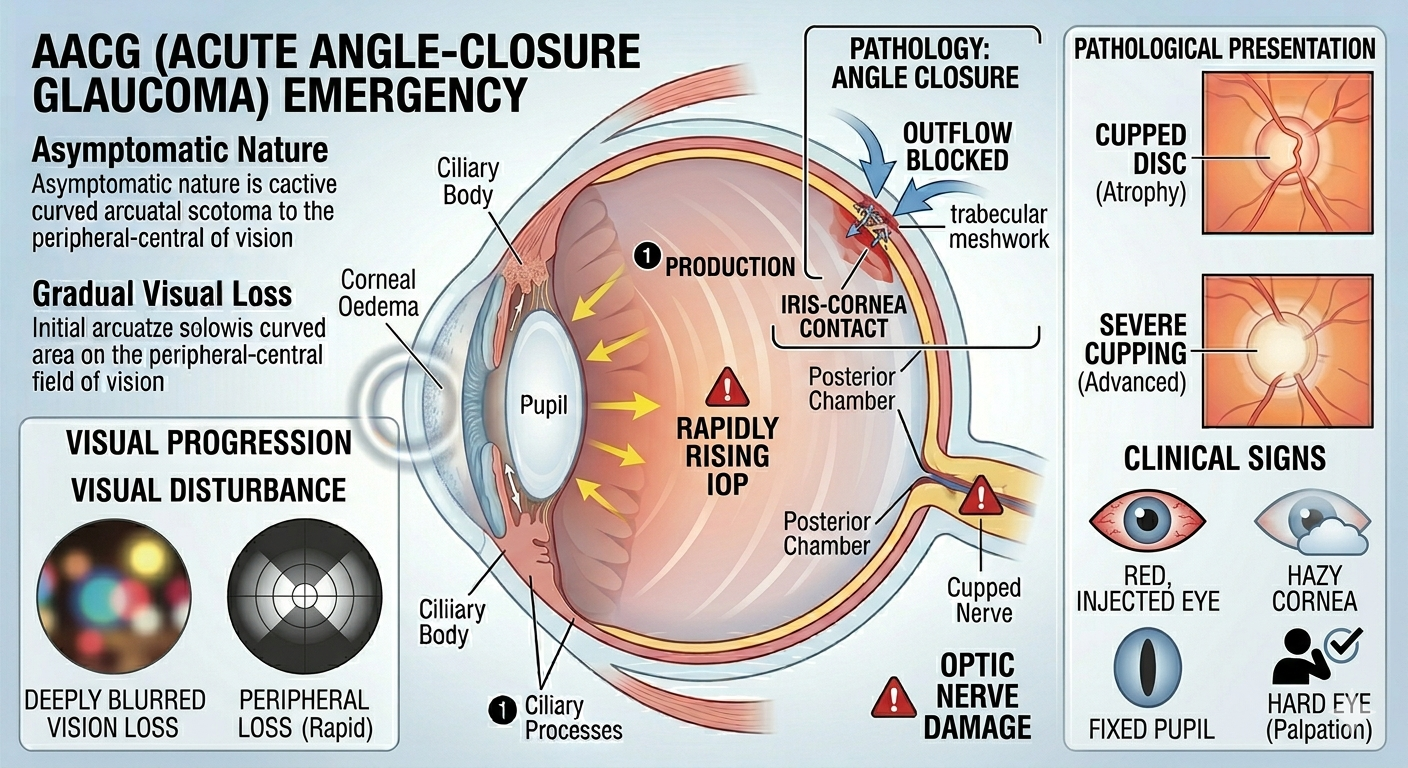
Acute Angle-Closure Glaucoma (AACG)
This is a medical emergency characterized by a rapid rise in intraocular pressure.
- Ocular Pain: Extremely severe, deep-seated pain in one eye.
- Systemic Symptoms: Often accompanied by nausea, vomiting, and severe headache, which can sometimes be misdiagnosed as an abdominal or neurosurgical emergency.
- Visual Disturbance:
- Sudden blurring of vision.
- Haloes around lights (caused by corneal oedema).
- Clinical Signs:
- Red Eye: The eye appears inflamed and injected.
- Hazy Cornea: The cornea becomes waterlogged/cloudy.
- Fixed Semi-dilated Pupil: The pupil is vertically oval and does not react to light.
- Shallow Anterior Chamber: The iris is positioned very close to the cornea.
- Hard Eye: Upon gentle palpation, the eye feels much harder than the unaffected eye.
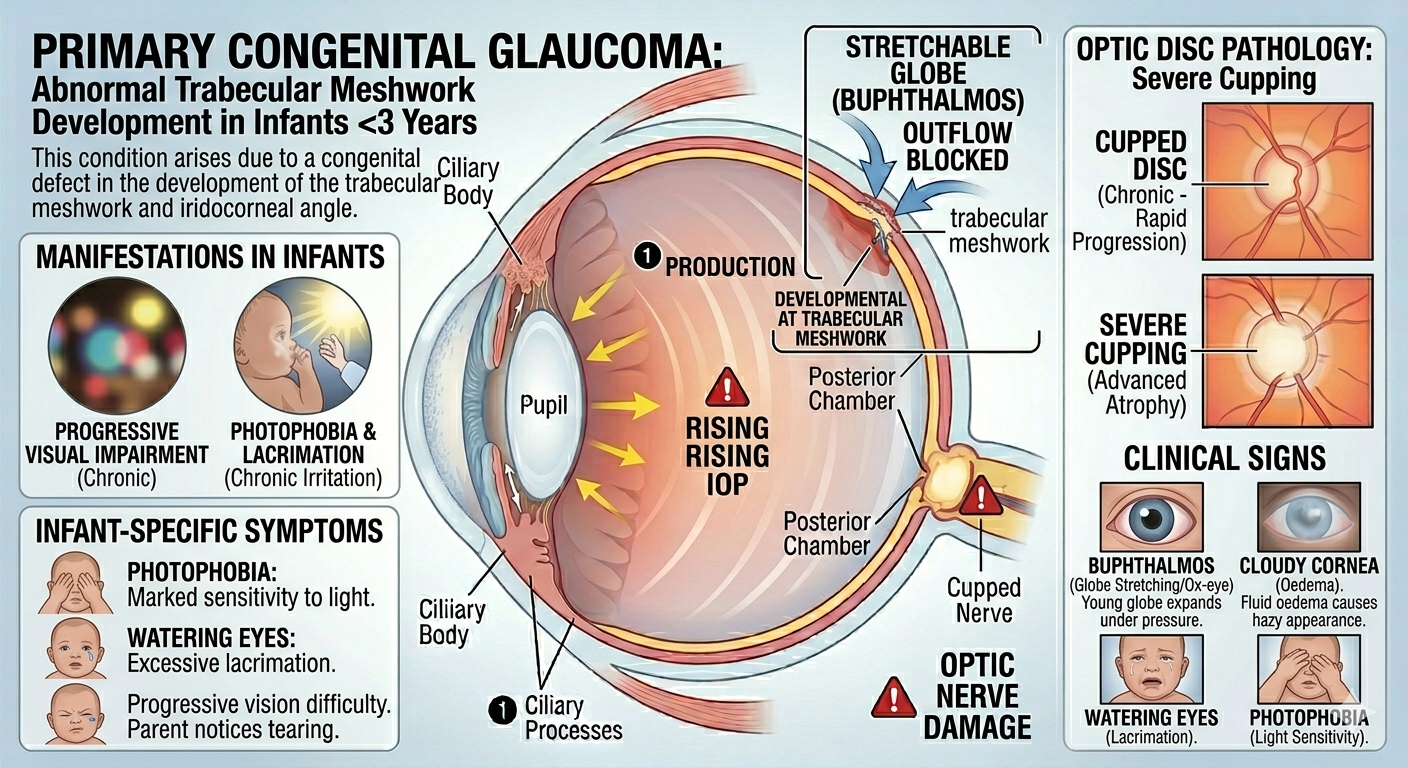
Primary Congenital Glaucoma
This occurs due to abnormal development of the trabecular meshwork in children under the age of three.
- Buphthalmos: Enlargement of the eye (also known as “ox-eye”) because the young globe can stretch under pressure.
- Cloudy Cornea: Oedema causes the cornea to appear hazy.
- Photophobia: Sensitivity to light.
- Watering Eyes: Excessive lacrimation.
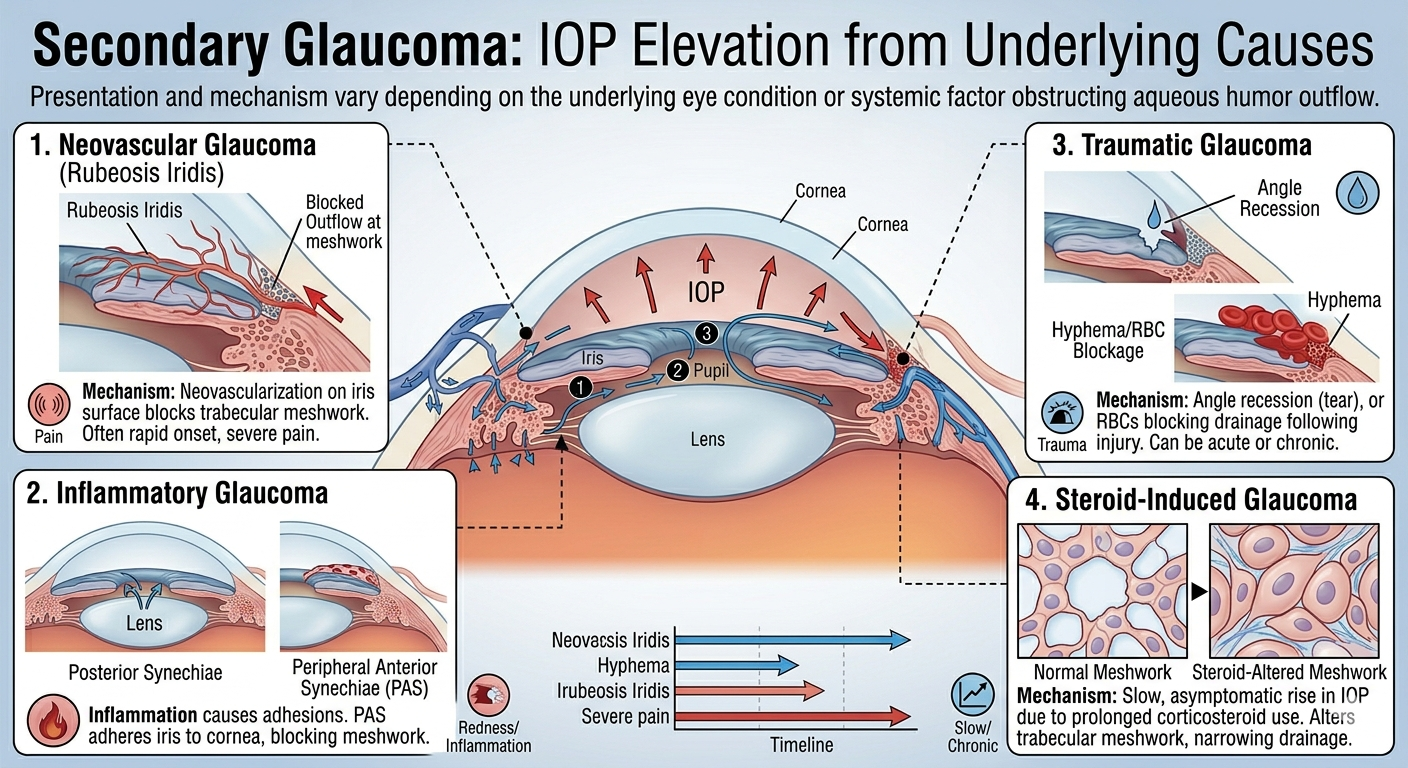
Secondary Glaucoma
Presentation depends on the underlying cause:
- Neovascular Glaucoma: Growth of new vessels on the iris (rubeosis iridis) which block the trabecular meshwork.
- Inflammatory Glaucoma: Inflammation causing posterior synechiae (adhesions between the lens and iris) or peripheral anterior synechiae (adhesions between the iris and cornea).
- Traumatic Glaucoma: Damage to the drainage angle or red blood cells blocking the trabecular meshwork following injury.
- Steroid-Induced Glaucoma: A slow, asymptomatic rise in IOP resulting from prolonged use of topical, inhaled, or systemic corticosteroids.